Select patient and Chart:
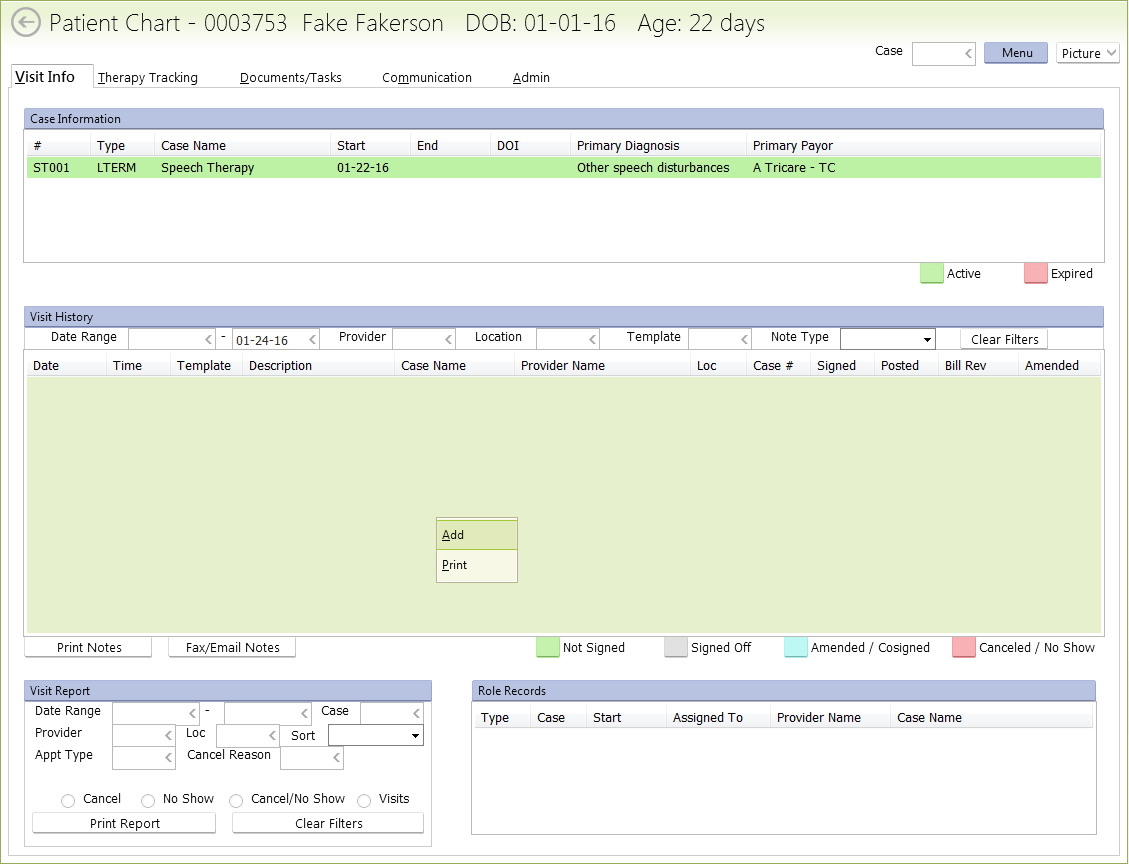
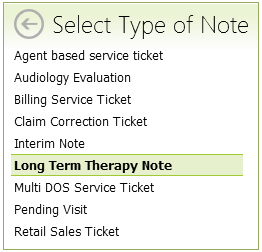
Select “Long Term Therapy Note“:
When the “Case List” for your patient appears:
- If there are no cases listed, contact staff ASAP to have a case created
- If there are multiple cases, be sure to select the case for your type of therapy (speech, OT, PT, feeding, etc)
- The case will most likely end with “001”, such as “ST001” or “PT001”.
- IF there is an “002” case, then contact office staff to be sure which one to select
When the “Initial Evaluation” screen pops up, in the upper-right corner:
- Make sure both the “Ther” and “Assigned” initials are your (the therapist) initials
- Change “Type” to “Initial Evaluation“
- Change “Eval” to either:
- SLT Standard
- OT Standard
- PT Standard

Now click the “Subjective” tab:
“Parent / Family Concerns (S)” area:
- In the text box, enter a few sentences of the parent / family concerns.
- Date of Illness / Onset: today’s date, unless there is an old eval use that date???
- Enter who brought the child to this evaluation
- Enter who the child lives with
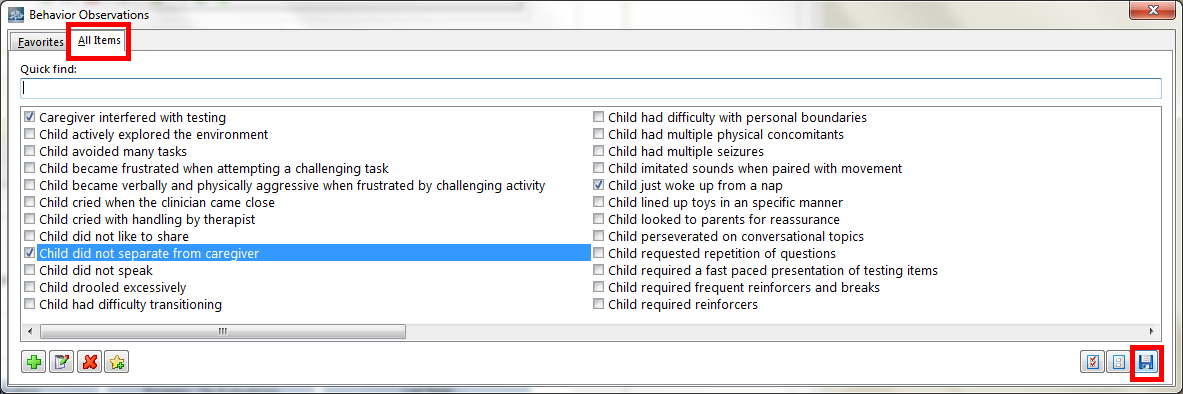
Behavior Observations:
- Click the green plus sign to add behavior observations
- You can click the “All Items” tab to select from more choices
- If you do not see a choice you need, contact office staff to have it added. (Do not attempt to add it yourself)
- When you are finished selecting observations, click the “Save” icon in the bottom-right
Reliability (S):
- Select if the observed behavior was an accurate (typical) representation of the child’s behavior.
“Area of Development Causing Concern“:
- Click the green plus sign, select concerns from yourself and parents, and click the “Save” icon in the lower-right
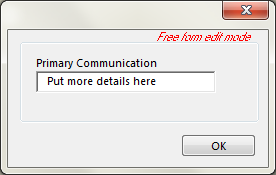
Primary Communication:
- Add communication concerns, and you can then double-click the concern to add more detail:
 Medical History:
Medical History:
- Medical History is “shared” information between all therapy types such as speech, OT, PT, feeding, etc.
- Some therapist prefer to complete the Medical History with the parents present